



QIPC Pulse – Quicklinks
- The 2026 influenza (flu) season is upon us!
- Influenza and its impact on our community
- Why are influenza vaccination rates not improving in children?
- Introducing FluMist for children aged 2 to 17
- How can Quality Improvement support FluMist vaccination uptake?
- Identifying children aged 2-17 who have not yet had a flu vaccination
- Helpful QI tips for health professionals
- References and additional resources
“Influenza is more serious than a common cold as it can, in severe cases lead to; pneumonia, inflammation of the heart or brain, or sepsis. Every year people in NSW die from flu-related illness.”
– New South Wales (NSW) Health, 2026
The 2026 influenza (flu) season is upon us!
Influenza is a highly contagious respiratory infection which is more serious than the common cold. It is a common cause of hospitalisation and in severe cases, can result in breathing difficulties, pneumonia or death. The most common influenza infections are caused by influenza ‘A’ and ‘B’ viruses, however there are various subtypes and strains.
The Australian Centre for Disease Control 2026 (Australian CDC) reiterates the influenza virus mutates easily with gradual changes through a process called antigenic drift. The ever-evolving virus is the main cause of seasonal outbreaks, hence the importance of staying up to date with annual vaccinations.
The National Centre for Immunisation Research and Surveillance (NCIRS) 2026 identified peak influenza activity in Australia varies each year but is most commonly active in May to September. Influenza has higher transmission rates in colder seasons as the virus can survive for longer periods outside of the host’s body. Despite known peak transmission periods, infection can still occur year-round.
Studies have proven without yearly influenza vaccination, antibodies begin to struggle to recognise newer strains of influenza over time. An unequipped immune system has a slower response rate to the virus, increasing the risk of severe complications.
The Australian CDC 2026 highlights influenza is a nationally notifiable disease which poses a risk to public health. The National Notifiable Diseases Surveillance System (NNDSS) coordinates data to identify trends in diseases, assesses the impact and provides reports to the World Health Organisation (WHO). Based on these reviews, the Australian Influenza Vaccine Committee (AIVC) recommends viral strains to be used for influenza vaccines in the Southern Hemisphere.
Influenza and its impact on our community
The best form of protection against influenza is getting vaccinated each year. Despite being a vaccine-preventable disease, it is one of the highest causes of hospitalisation in Australia.
The Australian CDC 2026 highlighted that each year influenza in Australia causes approximately:
- 3,500 deaths
- 18,000 hospitalisations
- 300,000 visits to a GP
The Australian Bureau of Statistics (ABS) 2026 reported in 2025 there were 1,744 deaths associated with influenza. This is a notable increase in comparison to 1,064 deaths in 2024 and 613 in 2023.
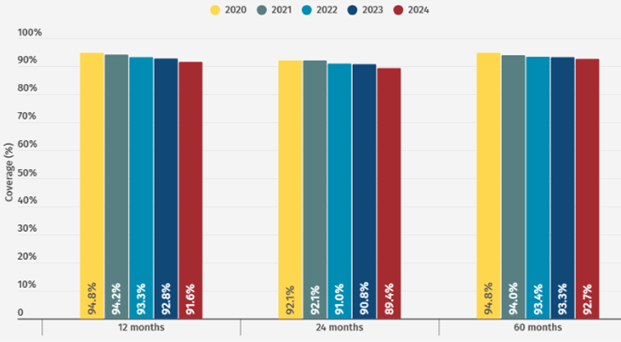
The NCIRS reported influenza vaccination rates and overall coverage continued to remain suboptimal across all age groups in 2025, despite being funded under the National Immunisation Program for specific eligible cohorts. In NSW, childhood and adolescent vaccination rates continue to decline, with the greatest decline seen amongst adolescents.
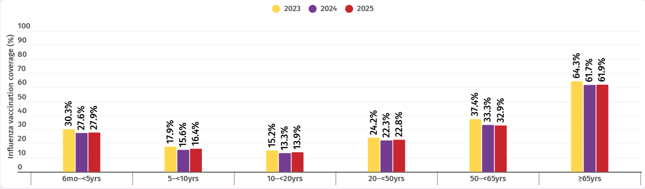
Figure 1 – Influenza vaccination coverage across all age groups, 2023-2025.
Annual Immunisation Coverage Report 2025 – Summary | NCIRS
Why are influenza vaccination rates not improving in children?
In 2019, the WHO placed vaccine hesitancy in the top 10 threats to global health.
Revisit our newsletter on vaccine hesitancy and discover quality improvement (QI) activities your practice can undertake to strengthen vaccine confidence and improve immunisation outcomes – QIPC Pulse – Vaccine Hesitancy
The National Vaccination Insights Project 2025 performed a recent study to identify childhood vaccination barriers for Australian parents which included:
- poor access to immunisation services
- low confidence in vaccination efficacy
- misinformation based on myths surrounding vaccination coverage and its importance
- mistrust in healthcare professionals providing information
- social influences
The 2025 national survey highlighted the highest acceptance barrier was negative belief toward the safety of vaccines. The second highest was a lack of trust in vaccine information from healthcare providers. The ongoing vaccine fatigue and decline in overall vaccine confidence was found to be more prevalent in parents of young children.
There is no singular solution or approach for vaccine hesitancy as the magnitude of negative beliefs, myths and mistrust must be addressed individually for each patient and/or parent.
In response to the notable decline in immunisation coverage across NSW, South Western Sydney PHN has launched an Immunisation Hero campaign. The campaign aims to support general practices in promoting immunisation uptake and boosting vaccination awareness within the community. For more information or resources, please visit our website.
Introducing FluMist – a needle-free vaccination for children aged two to 17 years
The NSW Nasal Spray Influenza Vaccination program introduced FluMist, a live attenuated influenza vaccine administered in each nostril (needle-free), to children aged two to 17.
Contrary to popular belief, the live attenuated influenza vaccine (LAIV) has been administered to millions of children in the Northern Hemisphere since 2003. Recent systematic studies show LAIVs are just as safe as inactivated influenza vaccines (IIV).
FluMist was added to the NSW vaccination program to explore if needle-free vaccinations can increase influenza immunisation coverage rates in children, while reducing the incidence of influenza and influenza-associated hospitalisations.
The Australian Government established 95 per cent as the minimum immunisation rate required to achieve herd immunity for many vaccine-preventable diseases. The Royal Australian College of General Practitioners (RACGP) reported in a recent publication that as of 16 May, only 15 per cent of children aged two-to-five years old had received a flu vaccine with 69 per cent of the vaccinated group receiving the needle-free option.

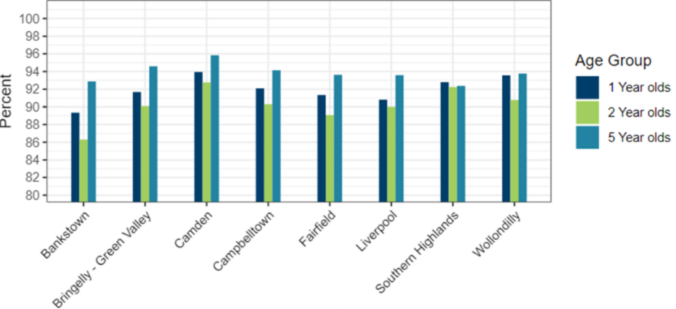
Figure 2 – LAIV administration in children and adolescents by age group, 2026 (YTD)
All children and adolescents: 2026 (YTD) administration of live attenuated influenza vaccine | NCIRS
Did you know?
FluMist contains a highly processed form of porcine gelatine to stabilise the live virus.
Gelatine used in live vaccines is highly purified and hydrolysed, so it is different from gelatine used in foods.
Religious authorities and representatives of Islamic and Jewish communities have issued guidance stating porcine-derived gelatine in vaccines is permissible.
If families or individuals prefer to avoid LAIV due to the porcine gelatine, they can have the traditional intramuscular vaccine as an alternative.
– New South Wales (NSW) Health, 2026
FluMist resources and additional information:
- NSW Nasal Spray Influenza Vaccination Program – Information for health professionals | NSW Health
- Nasal spray influenza vaccine – Information for families and carers | NSW Health
- Winter Respiratory Vaccination Toolkit | NSW Health
- How to talk about vaccines | WHO
How can Quality Improvement support FluMist vaccination uptake in your practice?
Quality Improvement plays a pivotal role in driving practice-based decisions to make changes, based on current evidence. POLAR is a user-friendly data extraction and analysis tool which can be used to support QI-based activities in your practice.
Ways POLAR can assist with QI:
- create a patient list within POLAR which identifies patients eligible for influenza immunisation – you can tailor your report to meet practice needs or a specific demographic
- use the extracted patient list to audit patient files and identify any gaps in clinical data
- use Walrus alongside your clinical information software system to further identify missing data within the practice
- for more information on Walrus, refer to the POLAR Walrus Tool Guide | South Western Sydney PHN
- track improvements in practice data quarterly in conjunction with Models for Improvement to compare baseline and current data
- collaborate with SWSPHN in quarterly QI meetings for a team-based QI approach and assistance in using POLAR or how to further improve practice data
Identifying children aged two to 17 who have not yet had an influenza immunisation
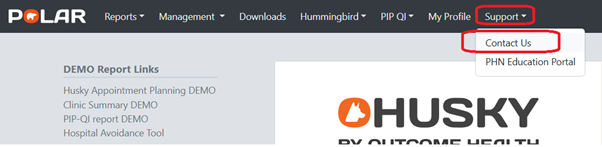
SWSPHN has various resources to assist your practice with QI activities. If you are unsure how to access POLAR, or need help with the initial use of POLAR, contact your Clinical and Quality Improvement (CQI) Officer or your PAO/PSO for more information.
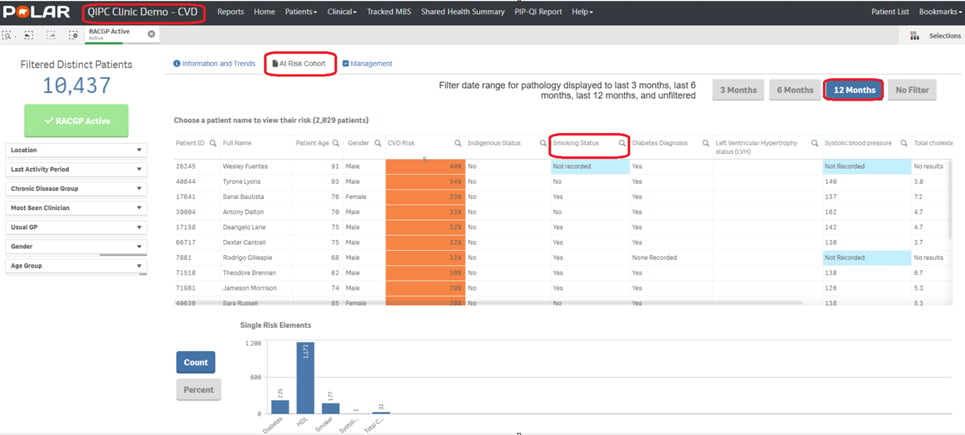
The SWSPHN CQI team have created the following MFI and POLAR walkthrough to assist practices in identifying patients aged two to 17 years.
Model for Improvement (MFI):
- Model for Improvement Template
- Model for Improvement Walkthrough
- Sample MFI – FluMist Vaccination | South Western Sydney PHN
POLAR Walkthrough:
Helpful tips for health professionals participating in QI
It is important to maintain accurate data in patient files – POLAR extracts data from the practice’s clinical information software. POLAR does not obtain data from AIR, My Health Record or PRODA.
What if my patient has had a vaccination elsewhere?
If immunisations were administered elsewhere, the practice can update a patient’s immunisation history within their patient records. Accuracy is ensured by using a patient’s AIR immunisation history.
SWSPHN has created a sample, editable Model for Improvement (MFI) to help practices implement processes to regularly update immunisation history using AIR:
Clinical information software walkthroughs to utilise AIR to maintain up to date patient records:
- Medical Director Walkthrough – Update Immunisation History via AIR | South Western Sydney PHN
- Best Practice Walkthrough – Update Immunisation History via AIR | South Western Sydney PHN
Private bookmark function:
The private bookmark function in POLAR allows users to save searches created with specific filters for future reference.
References and additional resources
- National survey shows declining vaccine confidence among parents | NCIRS
- 2026 vaccination guidelines for GPs: influenza, RSV and COVID-19 | South Western Sydney PHN
- NSW Nasal Spray Influenza Vaccination Program – Information for health professionals | NSW Health
- Influenza fact sheet | NSW Health
- Influenza (flu) | Australian Centre for Disease Control
- Deaths due to acute respiratory infections in Australia, March 2026 | Australian Bureau of Statistics
- 2025 national survey – childhood influenza vaccination barriers in Australia | NCIRS
- NSW expands eligibility for free FluMist vaccine | RACGP
- New research urges coordinated action to reverse Australia’s declining childhood vaccination rates | NCIRS
- Childhood vaccination barriers in Australia and strategies to address them | National Vaccination Insights Project
If you wish to find out more POLAR Puffin or SWSPHN’s QIPC program, please email cqisupport@swsphn.com.au or visit our website Quality Improvement in Primary Care.




 Why do we need MyMedicare registration?
Why do we need MyMedicare registration?








